|
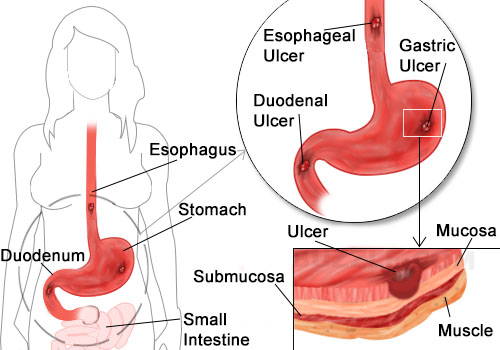
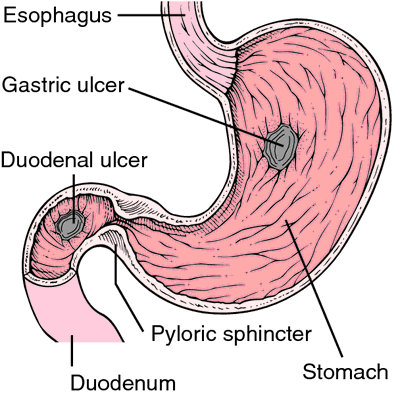
Peptic ulcers (an ulcer is an erosion of the tissue, producing a crater-like lesion) occur in the stomach (gastric ulcer) or the first portion of the small intestine (duodenal ulcer). Duodenal ulcers are more common, occuring in an estimated six to twelve percent of the adult population in the United States. In other words, approximately ten percent of the U.S. population has clinical evidence of duodenal ulcer at some time in their lifetime. Duodenal ulcers are four times more common in men than in women, and four to five times more common than gastric ulcers.
Although symptoms of a peptic ulcer may be absent or quite vague, most peptic ulcers are associated with abdominal discomfort noted forty-five to sixty minutes after meals or during the night. In the typical case, the pain is described as gnawing, burning, cramp-like, or aching, or as "heartburn." Eating or taking antacids usually results in great relief .
Even though duodenal and gastric ulcers occur at different locations, they appear to be the result of similar mechanisms. Specifically, the development of a duodenal or gastric ulcer is a result of damage to the protective factors that line the stomach and duodenum.
In the past, the focus has primarily been on the acidic secretions of the stomach a the primary cause of both gastric and duodenal ulcers. However, more recently the focus has been on the bacterium Helicobacter pylori and non-steroidal anti-inflammatory drugs.
Gastric acid is extremely corrosive. The pH of gastric acid (pH 1 to 3) would eat an ulcer right through the skin. To protect against ulcers, the lining of the stomach and small intestine has a layer of mucus, a slippery layer of mucus (mucopolysaccharides). In addition, the constant renewing of intestinal cells and the secretion of factors that neutralize the acid when it comes in contact with the stomach and intestinal lining also protect against ulcer formation. Gastric acid is designed to digest the food we eat, not the stomach or small intestine.
Therapeutic Considerations
Individuals who experience any symptoms of a peptic ulcer need competent medical care. Peptic ulcer complications such as hemorrhage, perforation, and obstruction represent medical emergencies that require immediate hospitalization. Individuals with peptic ulcer must be monitored by a physician, even if they are following the natural approaches discussed below.
Lifestyle Habits
Stress and Emotions
Stress is universally believed to be an important causative factor in peptic ulcers. However, this link is quite controversial in the medical literature. One of the big problems is that studies attempting to examine this assumption about stress and ulcers have been poorly designed. Several studies have shown that the number of stressful life events is not significantly different in peptic ulcer patients than in carefully selected, ulcer-free controls. These data suggest that it is not simply the amount of stress, but rather the patient's response to it, that is the significant factor. A large study of 4,000 persons who had no history of peptic ulcer disease revealed that those who perceived stress in their lives were at increased risk of developing peptic ulcers. For more please visit: www.HealingMoringaTree.com
0 Comments
By Healing Moringa Tree. Com
Large Leaf Mega Moringa Oleifera!
We at Healing Moringa Tree have extra large leaf Moringa Oleifera Species. After growing Moringa Trees for some time we has discovered that there are two types of Moringa Oleifera Species. Small leaf Moringa which grows slower and smaller leaves. 
Large Leaf Mega Moringa Oleifera!

Large Leaf Mega Moringa Oleifera!

Large Leaf Mega Moringa Oleifera!
Moringa Bundles Try our large or the small Moringa Tree Starter Kit, or choose from our Herbal Infusion Starter kits. We'll get you started on the right track, believe that!Top 10 Home Remedies for Cirrhosis of the Liver |




Get your Moringa Tree!

Archives
June 2019

We sell Organic Moringa Trees,Moringa seeds.Southern California source of healthy Organic Moringa Trees. 

Healthy Moringa shampoo!
Categories
All

infused moringa olive oil!



|

- Store Shop
-
MORINGA TREES & SEEDS
- MORINGA TREES
- Buy Moringa Seeds & Trees
- Moringa Tree Starter Kit
- Moringa Root Kits
- Wholesale Moringa Trees
- Organic Moringa Seeds
- Buy Oleifera Seeds >
- Buy Stenopetala Seeds
- Buy Moringa Roots
- Baobab Trees for Sale >
- Buy Medicinal Plants >
- Growing Moringa
- Sustainable Supplies >
- Moringa Books >
- Ground Organic Moringa seeds
- Non-Toxic ECO Moringa Cleaners
- Clay Tea Pots
-
Moringa Health
- ORGANIC HERBAL SMOKES
-
Moringa Powder, Capsules, Tea, Dried Leaves,
>
- Moringa Honey
- Moringa Alkaline Water
- Moringa Recipes
- Moringa First Aid kits
- Moringa Tooth Powder Kit
- Diatomaceous Earth
- Buy Turmeric >
- MORINGA SPAGYRIC TINCTURE >
- Fresh Moringa >
- Moringa Herbal Olis >
- Moringa Oral Care >
- Moringa Nail Polish
- Moringa Sample set
- Colloidal Silver Products
-
Moringa Beauty Products
- Mamas Moringa Baby Products
- Organic Moringa Cosmetic Products
- Aroma Herbal Mood Sprays
- Moringa Hair Products >
-
Moringa Skin Products
>
- Organic Moringa Oil >
- Moringa Soap
- Moringa Hand Soap
- Moringa Natural Skin Care System
- Moringa Anti-Aging Face Lotion
- Moringa Infused Clay Mask
- Roll on Aluminum-Free Moringa Herbal Deodorants
- Moringa Herbal Deodorants
- Moringa Sunscreen
- Moringa Bath Salt
- Moringa Hand Sanitizer
- Moringa Chest Rub
- Moringa Foot Spray
- Moringa Vaginal lubricant
-
Moringa For PETS
- Moringa Silky Coat Dog Grooming Products
- Yorkie Hypoglycemia Relief Multivitamin Drops
- Moringa American Staffordshire Terriers
- Moringa Healthy PETS
- Moringa Doggy Treats
- Moringa Dog Food
- Organic Moringa Cat Treats
- Organic Moringa Pigeon Feed
- Organic Moringa Fish food Flakes!
- Moringa Pet Body Products
- Moringa GIFTS
- Healing Moringa MASSAGE & SPA







 RSS Feed
RSS Feed
